Background to Cancer Survivorship
Globally, the incidence of cancer continues to rise with an aging population and with increasing rates of some cancers in younger populations (1,2). For Canada in 2024, there were 247,100 new cancer cases and 88,100 cancer deaths in 2024 (excluding non-melanoma cases) (3). The number of cancer survivors has also been growing substantially for many cancers with about 64% of people expected to survive at least five years after their diagnosis in 2024 (4). This was an increase from 55% in the early 1990s. The number of cancer survivors is expected to continue to rise due to new treatment modalities such as immunotherapy and other precision cancer or targeted treatments, which have improved survival rates for many cancers (5).
As this population has grown, we have learned from cancer survivors that the cancer experience does not end after treatment; and many survivors require long-term hormonal or maintenance therapy; or ongoing treatment for cancer control.
Furthermore, the cancer control continuum is not linear (prevention, detection, treatment, post-treatment/survivorship, end-of-life); instead, it is circular. Once patients are treated and cured, or their disease is in remission or stable, the focus of care must circle back to prevention, early detection and as needed, retreatment, until that individual either dies as a result of cancer or an unrelated cause (6). Consequently, the nature of cancer survivorship has changed over the last decade, whereby many survivors will be treated with curative intent (i.e. adjuvant breast cancer treatment and deemed cancer free), whereas others even those with advanced disease may experience ongoing periods of remission, relapse with re-treatment, or experience cancer as a chronic illness due to ongoing health challenges or as an advanced chronic disease and many will require life-long treatment to maintain disease control (hormonal therapy). Patients exposed to newer treatments (e.g. immunotherapy) or complex treatments (i.e. transplants) may experience unique long term and late effect challenges and health risks during post-treatment survivorship.
It is well known that cancer and cancer treatment have a substantial impact on the long-term health and quality of life of survivors. Cancer survivors are at risk of long-term and late effects that are dependent on the type of cancer, stage of cancer, and the therapies used to treat the cancer; and other risk factors such as age, genetics and social determinants of health (7,8,9). Common long-term and late effects of cancer treatment are shown in Table 1. Common Long-Term and Late Effects of Cancer Treatment.
The late and long-term effects experienced by survivors of cancer are diverse. Common long-term consequences can include cognitive dysfunction, pain, fatigue, sleep disturbances, sexual dysfunction, or issues with body image and/or sexuality/intimacy health concerns (7,8,9). Looking at the most common cancer types, disease-specific consequences associated with prostate cancer may include erectile, bladder, or bowel dysfunction (10), whereas lung cancer survivors may face difficulty with shortness of breath, fatigue, weakness or maintaining pulmonary hygiene (11). Female breast cancer survivors may experience lymphedema, premature menopause, fatigue, or sexual dysfunction (12). Colorectal cancer survivors may report bowel dysfunction, decreased sexual functioning, and issues around body image or colostomy management (13).
Psychosocial distress is also a prevailing problem for many survivors, depending on the nature of the disease and treatment, and other socio-demographic, psychological, and environmental factors. This can include mental health disorders (i.e. depression, generalized anxiety), uncertainty, fear of cancer recurrence, or anger, sexual health, body image, loss and grief, or coping that may affect many aspects of quality of life (14,15). Social issues affected by cancer survivorship may include changes in relationships, functional status, communication, or community involvement (16,17). Existential and spiritual distress are also commonly reported among cancer survivors (18). Additionally, cancer survivors may have practical concerns about return to work, and need information about system navigation, available resources and how to effectively self-manage long-term consequences (19,20). Many survivors have employment and financial concerns and need vocational rehabilitation and/or return-to-work coaching (21). According to a recent meta-analysis, cancer survivors were more likely to be unemployed than healthy controls and the unemployment rate was higher among breast, gastrointestinal, and gynaecological cancer survivors (22). As shown in this study, factors such as cancer site, clinical prognosis, treatment method, socio-economic status, and attributes of the work itself influenced the re-employment of cancer survivors. The financial burden, including direct and indirect costs, experienced by cancer survivors and their families has a substantial impact on individuals and financial distress is commonly reported (23). In Canada, out-of-pocket costs, such as drugs, home care, homemaking, complementary and alternative medicines, vitamins and supplements, family care, travel, parking, accommodations, and devices, were problematic for 20% of survivors, and more than one-third of survivors required family members or caregivers to take time off work (24,25); and many family caregivers have high levels of emotional distress/stress (26).
Many of these models of care are dependent on appropriate risk-stratification of patients/survivors to low, medium, or high for deciding the appropriate model of care although consensus is lacking on what clinical disease or other characteristics are critical for predicting risk (36). Rather than aiming for a ‘one size fits all model’ of survivorship care implementing the most appropriate model based on personalized care pathways, relevant to the human and financial resources of the health care setting as well as geography (rural/remote, urban or metropolitan city) and type of organization and/or cancer population volumes (i.e. academic, community-based, etc.) that can also improve health outcomes and equitable access (37).
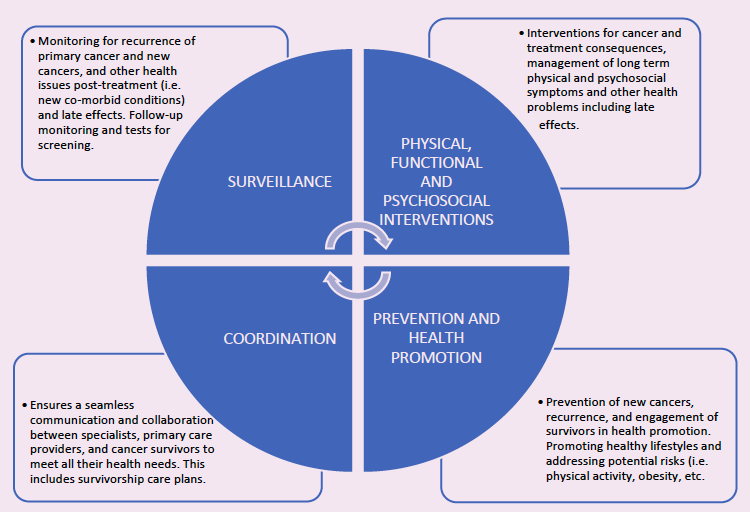
Regardless of the model of care, comprehensive and quality cancer survivorship care includes four essential components (Figure 1. Essential Components of Survivorship Care) as identified in the 2006, Lost in Transition Report from the landmark report of the Institute of Medicine and the National Council of Research (38), and revisited and updated in 2023 (39).
| Table 1. Common Long-Term and Late Effects of Cancer Treatment | ||
|---|---|---|
| Multidimensional Impact | Long-Term / Persistent | Late |
| Physical |
Fatigue Pain Neuropathy Endocrine issues Infertility Sexual health issues Cognitive impairment Disease specific issues Treatment specific issues Physical disability/impairment Change in weight loss/gain Bowel and bladder dysfunction |
Secondary primary cancer Cardiovascular disease Osteoporosis/endocrine issues Cataracts/other eye problems Oral health issues Sexual health impairment Metabolic syndrome Co-morbid disease e.g. diabetes Accelerated aging Pulmonary dysfunction Hearing loss Arthritis and joint problems |
| Psychosocial and Existential | Change in social connections/family/interpersonal relationships, existential issues, sense of purpose/meaning, sense of identity, change in spirituality, uncertainty, interruption of life/family goals. | |
| Mental Health | Depression, anxiety, post-traumatic distress, fear of recurrence, distress in family members and children. | |
| Vocational / Work Productivity | Professional identity, job change/loss, return to work distress and accommodation, work productivity. | |
| Financial / Insurance | Loss of financial stability/financial burden, concerns about health insurance, out of pocket costs. | |
Cancer treatment and depending on treatment exposures increase the risk for new primary or secondary cancers, and co-morbid conditions (e.g., heart disease, compromised bone health, endocrine disorders) that need to be prevented or mitigated (27). In addition, most cancer survivors are older and often present with co-morbid conditions at the time of cancer diagnosis; and cancer treatment may accelerate aging process resulting in cumulative and premature risks for other chronic conditions (28). Co-morbid conditions can also be exacerbated by cancer treatment and warrant special management in the context of health challenges related to multi-morbidity (29).
Thus, many survivors will have ongoing supportive care needs-physical, informational, emotional, psychological, social, spiritual, and practical – as a result of their experience of cancer, treatment exposures and dependent on the psychosocial and supportive care services they receive along the continuum (early survivorship and onwards) (30). The statement at the beginning of this chapter still rings true for many cancer patients as they transition to post-treatment survivorship, whereby many fall in the gap between acute and post-cancer treatment and report feeling unprepared, uncertain, low in confidence and vulnerable (31), and are unsure of how to navigate ongoing health challenges and learn to live well with and beyond cancer.
The growing population of cancer survivors alongside their health care and supportive care needs is placing unprecedented demands on human and financial healthcare resources and questions have been raised about the sustainability of the traditional oncology-specialist led model for post-treatment follow-up survivorship care (32,33). Typically, survivorship care has been provided by cancer specialists and has focused predominantly on surveillance and monitoring for disease recurrence (32, 33). Increasingly, is it recognised that survivors have other significant post-treatment supportive care needs that are poorly addressed (or are exacerbated at this point in the cancer trajectory) impacting on their quality of life, health and survival outcomes (34).
Several promising models of survivorship care are now emerging as possible alternatives to predominant models of oncologist specialist led-survivorship care including: 1) primary care-led, 2) shared-care, 3) nurse-led, and 4) patient-led/patient-initiated follow-up care with supported self-management with potential for cost-savings and improved access closer to home (33, 35). However, cancer care organizations may still be concerned about the equivalence of these models on clinical outcomes such as time to detection of recurrence and quality of life outcomes. An updated review of the evidence and recommendations regarding these models of care is warranted to inform end-user decision-making, health care providers and survivors and could serve as a catalyst for change and uptake of alternate models of care.
Other Essential Elements of Survivorship Care:
Additionally, early and ongoing access to multidisciplinary specialists to manage complex long-term health problems and prospective rehabilitation programs to mitigate or manage functional impairments and/or disability are also essential cross-cutting elements of survivorship care (40, 41). Moreover, there is international consensus that self-management support (SMS) should be a core component of early survivorship care services in routine cancer care (42) and across all survivorship models of care (48). Activation of survivors in chronic disease self-management and to reduce health risks through adoption of key healthy behaviours (i.e. tobacco cessation, alcohol consumption, healthy nutrition, weight and obesity management, physical activity/non-sedentary behaviour, sun safety and adherence to screening tests) is crucial to survival and wellness (43).
In developing this guideline, the guiding principles for ideal survivorship care were taken into consideration as foundational to the delivery of equitable survivorship care that is personalized to the individual and their health and supportive care needs (44). These principles were further refined from those identified through consensus in our 2011 guideline (45). These principles are as follows:
Care should be tailored to the personal needs of survivors and be sensitive to issues of religious and spiritual values, culture/race/ethnicity, language, gender, age, disability, living circumstance, geographic (rural/remote), literacy, and structural vulnerability.
Multidisciplinary and collaborative, involving a range of oncology specialists, primary care providers, nursing and allied health staff, as well survivors and their families.
Continuing medical care and support to transition from the acute setting to the community, using effective communication strategies, planned and coordinated FU.
Family, as defined by survivors, should be included in survivorship services; and engaged as active participants and collaborators in planning survivorship care.
Survivorship care should start from diagnosis and extend through treatment, post-treatment remission and/or ongoing maintenance therapy for cancer control and/or living with advanced disease as a chronic illness, palliative and end of life care
Psychosocial and supportive care services involve a range of disciplines, but are not limited to, nurses, oncologists, psychiatrists, psychologists, social workers, dietitians, rehabilitation providers, spiritual care providers, and primary care providers.
Essential components of survivorship services are not limited to psychosocial and supportive care but include the prevention of and surveillance for recurrent and new cancers, as well as clinical management of other late effects.
Survivorship services should focus on empowering survivors, with the support of their caregivers, to adopt self-management strategies and other behaviours necessary to optimize health and well-being inclusive of coaching on health promotion/prevention.
Survivors should be prepared early in the disease course for transition to the appropriate model of post-treatment care based on needs and health risks and facilitated by use of survivorship care plans
Evidence-based using guidelines and research, quality survivorship frameworks for service delivery, health policy that is outcomes focused, cost-effective and sustainable.
Figure 1. Essential Components of Survivorship Care